



The Knee
The normal knee is the largest and most complex joint in the body.
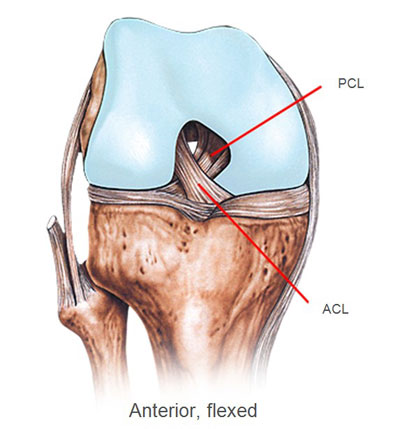
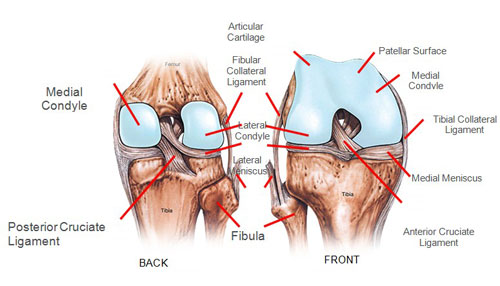
It is the articulation between the thigh bone (femur) and the shin bone (tibia). The front of the knee is protected by the knee cap (patella). The joint can be divided in to three areas, the inside (medial) compartment, the outside (lateral) compartment and the joint between the knee cap and the thigh bone (patello-femoral joint).
The joint surfaces are covered in articular cartilage. This is best thought of as stiff, sponge like material that contains water within its structure to provide a very smooth surface. Over years, the water content of the cartilage decreases and the surface can become damaged resulting in osteoarthritis.
The menisci or cartilages are two C shaped structures that lie on the upper surface of the tibia and act as shock absorbers. They are made of a slightly different material to the cartilage on the joint surface but, again, are dependent on a high water content to provide the cushioning function. With time, there is a tendency for dehydration to occur and the menisci can become stiffer and break up.
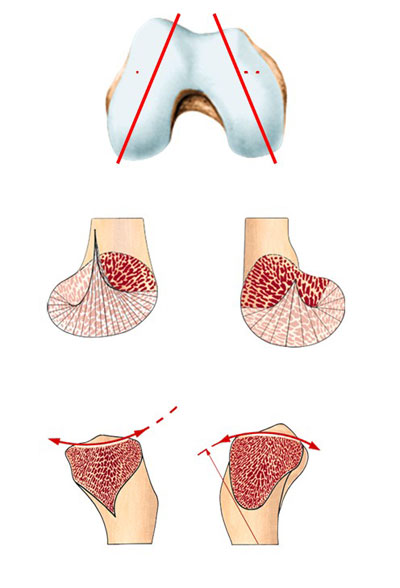
As you can see from the above diagram, the geometry of the knee joint is complicated, with the medial and lateral sides being of different length. This means that as the knee flexes the inside and outside halves move different amounts and produces some rotation. The design of a total knee replacement has to take this into consideration.
The upper surface of the tibia (shin bone) is different on the outside to the inside. The inside is concave and the outside is convex; this produces a degree of instability of the knee.
In the normal knee, this is controlled by both static and dynamic devices. The static devices include the ligaments, the joint capsule and the shape of the bones. The dynamic devices include the muscles and the menisci.
The consequence of this complexity is that not all of these features can be replicated in a total knee replacement. The picture below shows a knee replacement, there is a metal femoral part that resurfaces the femur, a metal tray with a spike that fits to the top of the tibia and the plastic insert that provides the articular surface.

When considering whether or when to undergo knee replacement surgery, it is important to be realistic about the outcome of such surgery. It is essential to understand that a "new knee" will function in a manner similar to that of a 65 year old's normal knee. That is to say that it will allow walking, swimming, skiing, golf, doubles at tennis, and cycling, but not impact activities such as running. It is possible to kneel after knee replacement. This may feel very odd because of the scar, but it will not harm the implant.
Most patients are very happy with the functioning of their new artificial knee. There does, however tend to be an increased incidence of dissatisfaction in younger patients, in whom, the knee replacement sometimes fails to meet their initial expectations. Prior to surgery, it is important to appreciate just what can and what cannot be achieved.
